| |
"Implementation of wireless biomedical sensors in advanced
clinical care"
Authors: Karl Oyri¹, Ilangko Balasingham¹,
Jan-Olav Høgetveit²
Speaker: Karl Oyri
Origin Institution:
¹ The Interventional Centre, Rikshospitalet University Hospital
² Department of Biomedical Engineering, Rikshospitalet University
Hospital
E-mail: karl.oyri@klinmed.uio.no
County: Norway
Post Address:
Karl Oyri
The Interventional Centre
Rikshospitalet University Hospital
0027 Oslo
Norway
Thematic: wireless technology, point of care data, invasive
blood pressure, biomedical sensor
Índice
general
Introduction
The Wireless Health and Care Project (WSHC) (1),
partly funded by the Norwegian Research Council, focuses on wireless
technology in healthcare. WSHC involves industrial-, research Institute-,
and clinical partners. The Interventional Centre (IVC) at Rikshospitalet
University Hospital in Oslo, Norway is one of the clinical partners.
As part of the WSHC Project, research was performed at IVC to evaluate
the use of wireless biomedical sensors in clinical practice. The
research hypothesis was that a difference between wired and wireless
pressure measurements was to be expected.
Methods
Sensor data from a modular wireless non-disposable piezoresistive
biomedical sensor prototype for continuous invasive blood pressure
measurement and continuous 2-channel ECG developed by MemsCap (2)
was compared with a state of the art patient monitoring system from
Siemens Medical utilizing disposable biomedical sensors from Edwards
Lifesciences (3). Measurements were performed in
a clinical trial involving four major laparoscopic surgical procedures.
The wireless standard Bluetooth (4) was used, as
investigated in an OR setting (5). High resolution
data from the two types of biomedical sensors were collected in
customized LabView applications (6) during the
surgical procedures and compared in MatLab (6)
statistically and sample-by-sample for visual inspection at a sampling
rate of 100HZ.
Results
We observed a very high rate of correlation between signal amplitudes
of the wireless and wired biomedical sensors during four laparoscopic
surgical procedures. This correlation is illustrated in Figure 1.
Discussion
Small changes in technology for invasive blood pressure measurement
have taken place last three decades (7). Transportation
of critically ill patients require adequate planning and monitoring
during transport (8 -10). Uninterrupted
wireless monitoring facilitates intrahospital patient transport.
Wireless monitoring replaces cables and reduce the potential risk
for adverse events related to disconnection (10).
Wireless technology also is battery driven, thus suitable for pre-hospital
patient monitoring. Traditional patient monitors are expensive and
operate on proprietary platforms, producing analog signals. Processing
of digital signals is of great interest in the point of care clinical
setting (11). The wireless biomedical sensor prototype
represents a low-cost, reliable and flexible alternative to traditional
signal transmission and data processing.
Conclusion
Wireless transmission of blood pressure data and EKG signals in
the OR is a stable, accurate and simple method with a potential
for developing new and cost-effective procedures, and to replace
traditional monitoring solutions based on cables.

Bibliography
(1)
Wireless Health and Care. http://www wshc no/ 2004 [cited 2004 Oct
30];Available from: URL: http://www.wshc.no/
(2) Wireless Physiological Pressure Transducer.
2004. Ref Type: Pamphlet
(3) Truwave PX 600F Pressure Monitoring Set. 2004.
Edwards Lifesciences Germany GmbH. Ref Type: Pamphlet
(4) Bluetooth. https://www bluetooth org/ 2004 [cited
2004 Oct 30];Available from: URL: https://www.bluetooth.org/
(5) Wallin MK, Wajntraub S. Evaluation of Bluetooth
as a replacement for cables in intensive care and surgery. Anesthesia
& Analgesia 2004 Mar;98(3):763-7.
(6) National Instruments. http://www ni com/ 2004
[cited 2004 Nov 8];Available from: URL: http://www.ni.com/
(7) Craft RL. Trends in technology and the future
intensive care unit. [Review] [65 refs]. Critical Care Medicine
29(8 Suppl):N151-8, 2001 Aug;29.
(8) Szem JW, Hydo LJ, Fischer E, Kapur S, Klemperer
J, Barie PS. High-risk intrahospital transport of critically ill
patients: safety and outcome of the necessary "road trip".
Critical Care Medicine 1995 Oct;23(10):1660-6.
(9) Velmahos GC, Demetriades D, Ghilardi M, Rhee
P, Petrone P, Chan LS. Life support for trauma and transport: a
mobile ICU for safe in-hospital transport of critically injured
patients. Journal of the American College of Surgeons 2004;199(1):62-8.
(10) Smith I, Fleming S, Cernaianu A. Mishaps during
transport from the intensive care unit. Critical Care Medicine 1990
Mar;18(3):278-81.
(11) Celi LA, Hassan E, Marquardt C, Breslow M,
Rosenfeld B. The eICU: it's not just telemedicine. Critical Care
Medicine 2001 Aug;29(8 Suppl):183-9.
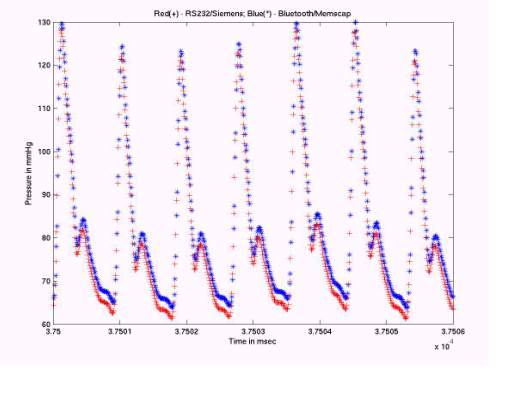
Figure
1: Wired and wireless blood pressure samples.
|

